
Winkelwagen
U heeft geen artikelen in uw winkelwagen
Compound blue nevus had clinical and histological similarities with other heavily pigmented melanocytic tumor, like the pigmented epithelioid melanocytoma. Distinctive genomic aberrations have allowed differentiating it. The defining characteristic of blue nevi family is the presence of activating mutations in the G protein α‐subunits, GNAQ and GNA11.
The particular clinical, histologic, and molecular features allow to differentiate compound blue nevus from pigmented epithelioid melanocytoma suggest that the latter does not belong to the BN family despite the microscopic resemblance.
1 Division of Dermatology, Internal Medicine Department - Medical School of Ribeirão Preto - Universidade de São Paulo- Ribeirão Preto (SP) -Brazil.
2 Department of Pathology - Medical School of Ribeirão Preto - Universidade de São Paulo- Ribeirão Preto (SP) -Brazil.
2 Department of Pathology - Medical School of Ribeirão Preto - Universidade de São Paulo- Ribeirão Preto (SP) -Brazil.
1 Division of Dermatology, Internal Medicine Department - Medical School of Ribeirão Preto - Universidade de São Paulo- Ribeirão Preto (SP) -Brazil.
1 Division of Dermatology, Internal Medicine Department - Medical School of Ribeirão Preto - Universidade de São Paulo- Ribeirão Preto (SP) -Brazil.
1 Division of Dermatology, Internal Medicine Department - Medical School of Ribeirão Preto - Universidade de São Paulo- Ribeirão Preto (SP) -Brazil.
2 Department of Pathology - Medical School of Ribeirão Preto - Universidade de São Paulo- Ribeirão Preto (SP) -Brazil.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License which permits unrestricted non-commercial use, distribution, and reproduction in any medium provided the original work is properly cited.
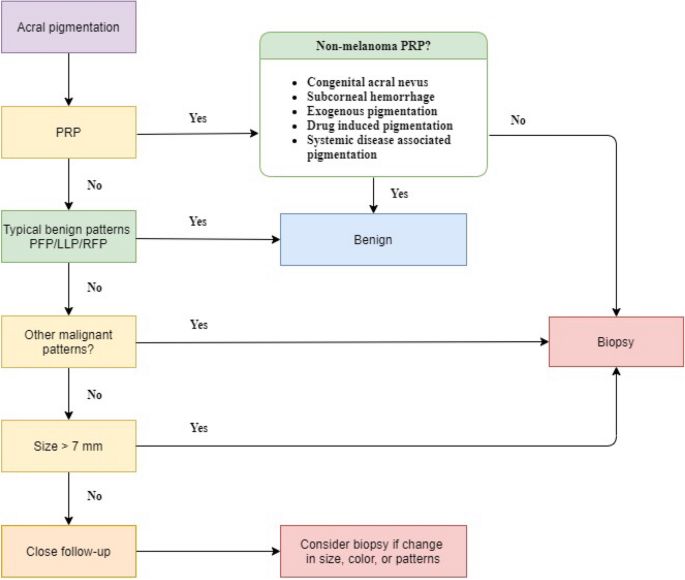
Dermoscopy has revolutionised clinical diagnosis of ALM by enabling detailed morphologic analysis of pigmented patterns. In this study, we found that grey colour, PRP, and IDP were significantly less common in small ALMIS than in large ALMIS (P = 0.002, P = 0.035, and P = 0.001, respectively).
PRP is the cardinal dermoscopic feature of ALM 9,10,17,19 . It is defined as prominent band-like pigmentation on the ridges of the dermatoglyphic lines 10 . Although it is the most well-known important dermoscopic features of ALM, PRP was absent in four cases of the small group (36.4%) in our data. Upon further analysis of small ALMIS without PRP, they showed other malignant features: irregular dots and globules in three, irregular fibrillar pattern in two, and IDP in one. Therefore, careful investigation of melanoma-specific dermoscopic patterns in addition to PRP is important especially in small lesions. IDP with variable shades from tan and grey to black colour is also specific to ALM 10,17 . Thirteen cases (61.9%) had IDP. This pattern was more prevalent in large lesions.
Early detection is crucial in improving melanoma prognosis. Saida and Koga proposed that a cut-off of larger than 7 mm is a helpful clue for ALM and incorporated this criterion in the three-step algorithm for early ALM screening 20 . Nonetheless, as ALMs generally arise de novo 9,21 , recognising small evolving lesions is essential for adequate management. However, the current literature on this topic is scarce. Data from Mayo clinic suggested that 6-mm acral melanomas could be missed when using the three-step algorithm 22 . Moreover, we reported two exceptional cases of evolving small ALMIS (4.5 mm and 5 mm). The cases were initially difficult to diagnose because they showed non-typical patterns. However, follow-up dermoscopic examination revealed increase in size and changing dermoscopic patterns. These cases highlight the importance of detecting small evolving pigmented macules for optimising ALM management.

Blue nevus is a benign melanocytic lesion whose most frequent variants are dendritic (common) blue nevus and cellular blue nevus. Atypical cellular blue nevus presents an intermediate histopathology between the typical and a rare variant of malignant blue nevus/melanoma arising in a cellular blue nevus. An 8-year-old child presented a pigmented lesion in the buttock since birth, but with progressive growth in the last two years. After surgical excision, histopathological examination revealed atypical cellular blue nevus. Presence of mitoses, ulceration, infiltration, cytological atypia or necrosis may occur in atypical cellular blue nevus, making it difficult to differentiate it from melanoma. The growth of blue nevus is unusual and considered of high-risk for malignancy, being an indicator for complete resection and periodic follow-up of these patients.
Keywords: Melanoma, Nevus, blue, Nevus, pigmented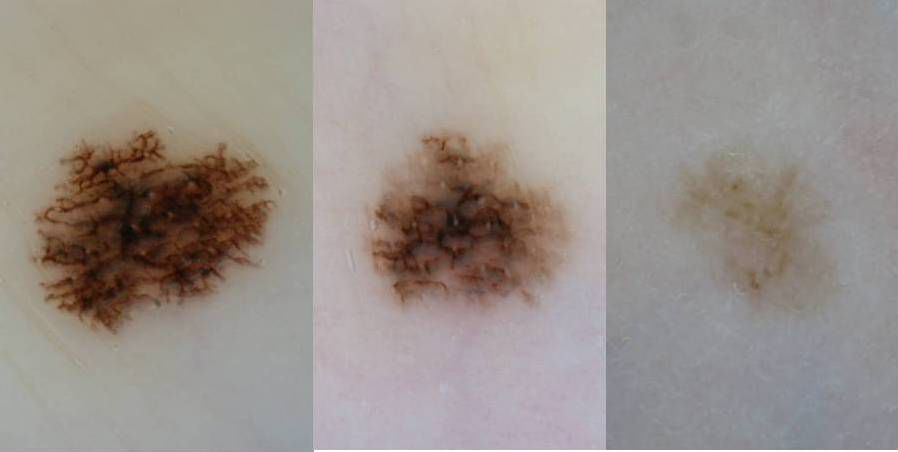
Medical News Today has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical journals and associations. We only use quality, credible sources to ensure content accuracy and integrity. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
Share this article

A blue nevus is a benign type of mole. It may appear as a blue lump on the skin. A blue nevus may be present at birth or develop as a person ages. Healthcare professionals refer to more than one blue nevus as blue nevi.
There are several different types of blue nevi. Common blue nevi are benign and will remain unchanged throughout a person’s life. However, there is a rare chance that a cellular blue nevus may change into a form of melanoma.
In this article, we look at the causes and risks of a blue nevus and discuss when to get advice from a doctor.
The main characteristics of a common blue nevus include:
Another type of blue nevus, the cellular blue nevus, differs slightly in appearance. In comparison with the common blue nevus, the cellular blue nevus is more likely to:
A blue nevus tends to occur as a solitary mole, which means that a person is unlikely to have more than one in a particular area of the skin.
Blue nevi can occur anywhere on the body, but they are most common on the:
The type of blue nevus will determine how and where it presents. The different types include:
A blue nevus does not usually require investigation. However, people should examine their skin regularly to check for any subtle changes to the mole, which may signal early signs of cancer.
If a doctor needs more evidence, they may use a dermatoscopy to check for a pattern consistent with a blue nevus. If a dermatoscopy is insufficient to diagnose a blue nevus, a doctor may perform an excision biopsy.
