
Winkelwagen
U heeft geen artikelen in uw winkelwagen
Secondary polycythemia is due to an increased level of EPO or other transcription factors that, in turn, lead to an increase in the production of RBC mass. It should be noted that, unlike primary polycythemia, there is no intrinsic defect in the erythroid progenitor cell lineage. The increase in the levels of EPO can be due to a number of factors, including genetic and acquired, which are discussed below.[5][6]
Classification of Polycythemia
On the basis of the response of the erythroid progenitor cells to the circulating cytokines, polycythemia can be further classified into primary or secondary.[8][1]
Primary Polycythemia
Primary erythrocytosis is due to the increased proliferation of erythroid progenitor cells secondary to an intrinsic cellular defect. These patients have a suppressed erythropoietin level.[1][4][6] It is of two main types.
Pure erythrocytosis: The subset of patients with pure erythrocytosis have an isolated elevated RBC mass in the absence of any other precipitating factor.[1]
Secondary Polycythemia [4] [6] [9]
Right-to-left cardiopulmonary vascular shunts, cyanotic heart disease[8] Hypoventilation syndromes including obstructive sleep apnea, obesity hypoventilation syndrome[7] Renal disease (local renal hypoxia, renal artery stenosis) Oxygen sensing pathway gene mutations (EpoR,3 VHL,8-10 and PHD216)[5][11]Tumors with excessive production of erythropoietin or erythropoietin related factors (renal cell carcinoma, hepatocellular carcinoma, pheochromocytoma, cerebellar hemangioblastoma, uterine leiomyoma, ovarian carcinoma, meningioma, parathyroid carcinoma/adenomas)
Drug associated: erythropoietin administration, androgen administration[13]Renal diseases including cysts, polycystic kidney disease, hydronephrosis, nephrotic syndrome, diffuse parenchymal disease, Bartter’s syndrome, end-stage renal disease, long-term hemodialysis, post-renal transplant erythrocytosis)
Eine Polycythaemia vera kann kausal bzw. kurativ bislang lediglich durch eine Stammzelltransplantation therapiert werden. Da ein solcher Eingriff mit einem hohen Risiko für Folgeerkrankungen und erhöhter Sterblichkeit einhergeht, wird dieser in aller Regel erst im stark fortgeschrittenem Erkrankungsstadium erwogen.
Demgegenüber stehen palliative Therapiemaßnahmen, die auf eine Reduzierung des Risikos für thromboembolische Ereignisse, Beschwerdelinderung sowie Verhinderung von Komplikationen abzielen, im Vordergrund der Behandlung einer Polycythaemia vera. Hierzu wird zur Reduzierung des Hämatokritwertes normalerweise eine Aderlasstherapie (Phlebotomie) eingeleitet, die eine schnelle und effektive Reduzierung des Blutvolumens gewährleistet.
Zu Beginn wird in Abhängigkeit vom spezifisch vorliegenden Hämatokritwert in zwei- bis dreitägigen Abständen eine Phlebotomie durchgeführt, wobei sich der Abstand zwischen den einzelnen Behandlungen im weiteren Behandlungsverlauf vergrößert. Zur Minimierung des Thromboserisikos und zur Behandlung der Mikrozirkulationsstörungen kommt gleichzeitig ein Thromboseaggregationshemmer (niedrigdosiertes ASS) zum Einsatz.
In manchen Fällen, bei welchen eine gezielte Reduzierung der Thrombozytenzahl angezeigt ist, kann Anagrelid, das suppressiv auf die Thrombozytenreifung wirkt, zur Therapie einer Polycythaemia vera appliziert werden.
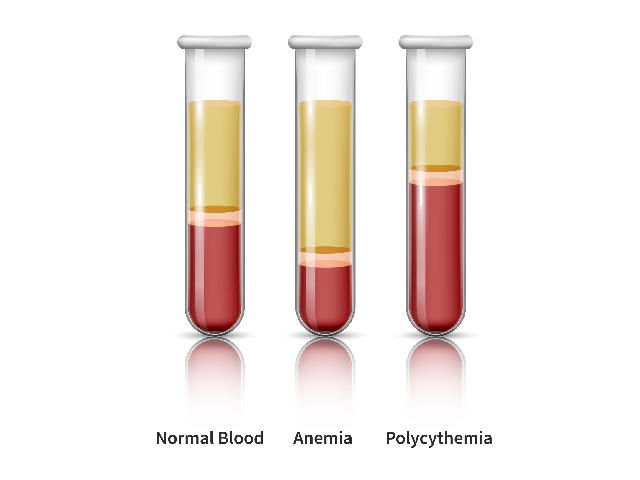
The percentage of blood volume that is composed of red blood cells is known as the hematocrit. For those living with polycythemia vera, the goal of treatment is to maintain a hematocrit below 45%.
To ensure that they stay below that level, people with polycythemia vera regularly visit their doctor to check their hematocrit. If it’s too high, they then undergo therapeutic phlebotomy—a process akin to blood donation—in which a large needle is inserted into a vein to remove blood from the body. The process takes anywhere from 10 to 30 minutes, according to Dr. Kremyanskaya, but the office visit in total can stretch much longer and interfere with people planning their lives.
People with polycythemia vera who are more likely to have problems like blood clots may receive additional treatments to reduce their red blood cell counts. But these treatments also have downsides, including low blood counts and infections. The bottom line, Dr. Kremyanskaya said, is that, beyond phlebotomy, “there are actually very few treatment options.”

Polycythemia vera is a medical condition that causes the body to make too many red blood cells. It is classified as a type of cancer. The excess red blood cells can cause dangerous complications such as blood clots, but the red blood cells do not invade healthy tissue. Polycythemia vera can progress to myelofibrosis or acute myeloid leukemia, which are aggressive types of cancer.
This condition can be treated with medical interventions and medication to reduce the effects of complications and improve life expectancy. Since there is no cure, disease surveillance and treatment have to be continued long term.
This article will discuss the life expectancy for polycythemia vera with or without treatment, and what treatments may be offered.
Als Polycythaemia vera wird eine chronische myeloproliferative Erkrankung bezeichnet, bei welcher eine erhöhte Synthese sämtlicher Blutkörperchen, insbesondere der Erythrozyten, im Knochenmark vorliegt.
Infolge dieser progredienten und irreversiblen Überproduktion wird eine Zunahme des Hämatokrits (zelluläre Blutbestandteile) sowie der Blutviskosität (Zähflüssigkeit) bedingt, die zu Mikrozirkulationsstörungen und einem erhöhten Risiko für thromboembolische Ereignisse führt.
Zudem werden bei der Polycythaemia vera zwei klinische Stadien differenziert. Die erste Phase ist durch eine erhöhte Erythrozytensynthese sowie Erythrozytose (erhöhte Erythrozytenzahl) charakterisiert und kann vollkommen symptomlos verlaufen. Die progrediente Spätphase zeichnet sich durch eine sekundäre Markfibrose (Markgewebsfibrose) mit extramedullärer Hämatopoese (Blutbildung außerhalb des Knochenmarks) sowie Splenomegalie (Milzvergrößerung) aus.
Ebenso können sich aus der Polycythaemia vera eine Myelodysplasie, bei welcher die Blutbildung zunehmend von mutierten Stammzellen übernommen wird, oder eine akute myeloische Leukämie entwickeln.