Winkelwagen
U heeft geen artikelen in uw winkelwagen
At this time, there are no published guidelines on the management and follow-up of PDS. 9 However, general management guidelines for soft-tissue sarcomas may be used for reference. Surgical treatment with wide location excision remains the first-line therapy for PDS. 4 Although specific guidelines for margin control are not well established, recent data suggest that 95% of cutaneous undifferentiated pleomorphic sarcoma tumors can be cleared with uniform peripheral surgical margins of 3 cm. 10
The potential for metastases and recurrence vary significantly among PDS and AFX. For PDS, the rate of metastasis is between 8.8% and 20%, whereas AFX has a metastatic potential of 1% to 2%. 4 Following treatment, the PDS recurrence rate is 17% to 35%, whereas AFX has a recurrence rate of 4.6% to 11.3%.
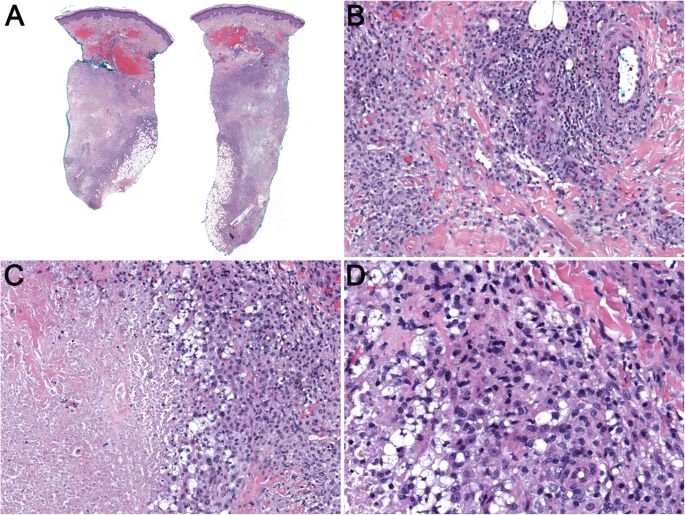
We present a case of PDS occurring on the scalp of a 72-year-old male patient, successfully treated with wide local excision. This case highlights the morphologic and histologic characteristics of PDS and discusses what is known about the management of this uncommon malignancy.
Naast de zeer frequent voorkomende basaalcelcarcinomen en plaveiselcelcarcinomen worden incidenteel ook andere typen niet-melanoom huidkanker geconstateerd. Denk hierbij aan het merkelcelcarcinoom (MCC), adnexcarcinomen, bepaalde types cutane lymfomen en allerlei soorten sarcomen van de huid. Bijna bij al deze tumoren wordt er initieel niet tot nauwelijks gedacht aan deze aandoeningen. [1,2] Bovendien komen veel van de zeldzame vormen van huidkanker vooral voor bij mensen die al bekend zijn met ‘gewone’ vormen van huidkanker, zoals bij solide orgaantransplantatiepatiënten en mensen met ernstig actinisch beschadigde huid. Toch is het belangrijk aan deze tumoren te denken, omdat het gedrag van veel van deze vormen van huidkanker anders is en veelal agressiever. Zodoende is verder onderzoek en aanvullende therapie regelmatig geïndiceerd.
Deze heterogene groep tumoren, die afkomstig is van de hui- dadnexen, presenteert zich vaak in het hoofd-halsgebied. Het is een zeldzame groep, met een geschat aantal nieuwe gevallen per jaar in Nederland rond de tachtig en vooral bij mensen op hoge leeftijd. Ook voor deze groep geldt dat er zelden initieel gedacht wordt aan een maligne adnextumor. [1] Deze tumoren hebben geen specifieke klinische kenmerken, kunnen op andere soorten niet-melanoom kanker lijken en omdat ze zeldzaam voorkomen kunnen zowel de clinicus als de patholoog hiermee moeilijk ervaring opdoen. Daarom is ook de histologische diagnose soms (zeer) lastig. Toch is het belang van duidelijke onderlinge differentiatie en juiste diagnose groot omdat de kans op (lokale) recidieven en metastasering ver- schilt. Daarnaast moet er ook gedacht worden dat sommige van deze adnexcarcinomen in het kader van bepaalde erfelijke aandoeningen kunnen voorkomen, zoals talgkliercarcinomen in Llynch/Muir-Torre en spiradenocarcinomen in brooke- spieglersyndroom.
Een van de meest voorkomende uit de groep apocriene- eccriene carcinomen (figuur 1) is het microcysteus adnexcarcinoom dat notoir lastig kan zijn om lokaal volledig te verwijderen. Vanwege hoge recidiefkans (> 50%!) wordt mohschirurgie dan ook regelmatig geadviseerd. Hierbij is een belangrijke valkuil de verwarring met het benigne plaquetype syringoom dat kan leiden tot overbehandeling. [12]
We present an unusual case of multifocal PDS arising in the areas of alpha-1-antitrypsin deficiency (A1AD) panniculitis in a lung transplant patient. We hypothesize that chronic, multifocal inflammation in the skin in the setting of immunosuppression led to simultaneous malignant transformation in numerous skin lesions. We discuss the challenges of diagnosing PDS, the therapeutic options, and stress the need for multidisciplinary management of these cases. To the best of our knowledge, this is the first report of a multifocal presentation of PDS. The unusual circumstances of this case shed light on the disease pathogenesis.
A 58-year-old white woman with a history of emphysema and chronic obstructive pulmonary disease (COPD) secondary to A1AD, who received lung transplantation 4 years prior, presented to dermatology with a 1-year history of painful nodules on the extensor surfaces of her upper extremities and back. She reported a 14-year one pack/day smoking history as well as fatigue, shortness of breath, cough, allergies, arthritis, leg swelling, muscle weakness, colitis, decreased appetite, nausea, light sensitivity, eye pain, and eye redness. She also reported depression and anxiety. She denied alcohol or drug use. She had completed high school and was now supported on disability. She also received emotional support from her husband who accompanied her to appointments and was involved in her healthcare. She had a family history of a cousin with cancer (type not reported). Following lung transplantation, she had been maintained on an immunosuppressive regimen of mycophenolate mofetil (MMF), tacrolimus, intermittent steroids, and a human alpha-1 proteinase inhibitor. Her post-transplant course was complicated by multiple respiratory viral and fungal infections, recurrent acute cellular rejection and lymphocytic bronchiolitis, chronic allograft dysfunction, recurrent lower extremity deep venous thrombosis, and an intermittent requirement for increases in her immunosuppressive therapy.