
Winkelwagen
U heeft geen artikelen in uw winkelwagen
Dermatitis herpetiformis adalah ruam lepuh kronis yang sering terjadi pada penderita penyakit celiac. Dermatitis herpetiformis umumnya menimbulkan keluhan berupa ruam yang disertai gatal atau sensasi terbakar di kulit. Dermatitis herpetiformis, atau disebut juga dengan penyakit Duhring, merupakan penyakit yang langka. Kondisi ini terjadi pada 10–25% penderita penyakit celiac. Gejala dermatitis herpetiformis biasanya mereda ketika penderitanya menjalani pola makan bebas gluten.
Di samping masalah pada gigi, dermatitis herpetiformis juga dapat menyebabkan masalah pencernaan berupa:
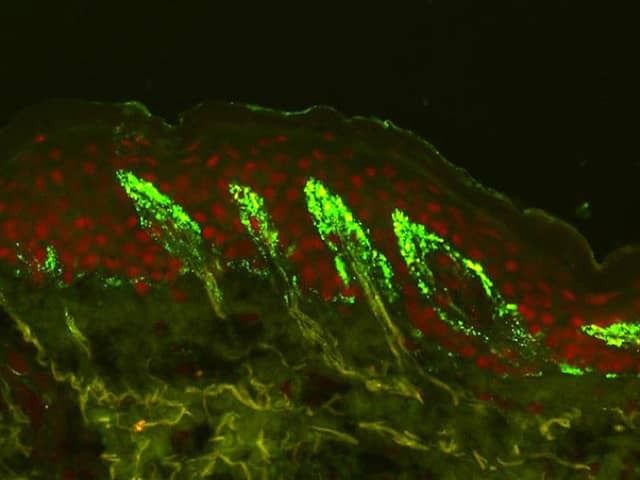
The histopathology of an intact vesicle in dermatitis herpetiformis demonstrates subepidermal blister formation with neutrophils located at the tips of the dermal papillae. There is frequently perivascular inflammatory cell infiltrate. Because vesicles may not survive the pruritis, clefting within the lamina lucida may not be seen.
Presentation
The characteristic lesions of dermatitis herpetiformis are grouped erythematous papules and vesicles located over extensor sites. Because the condition is so pruritic, intact vesicles are rarely seen, and the patient may simply present with excoriations. Lesions tend to be symmetrical and heal without scarring. Patients may develop punctate purpura on the palms and soles. Mucosal change may occur, and dental abnormalities have been reported, particularly enamel pits. Interestingly, first-degree relatives of a patient with GSE may also show enamel defects.

A gluten-free diet for life is strongly recommended in patients with DH, as it:
It may take up to 2 years for a gluten-free diet to reach its maximal effect.
Dapsone is the treatment of choice for DH, as it usually reduces itch within 3 days.
If intolerant or allergic to dapsone, the following may be useful:
There are reports that combination therapy with dapsone and sulfasalazine may be effective in patients who do not tolerate increasing doses of dapsone monotherapy.
Topical dapsone 5% gel was also shown to be effective as an adjuvant treatment for DH. Compared to oral dapsone, topical dapsone was associated with a lower lymphoma is increased in DH, the overall disease mortality is lower than the general population, possibly due to a reduction in cardiovascular disease and obesity.

You may need to see several specialists to help you manage your condition. For instance, a gastroenterologist can help with your digestive issues, and a dermatologist can help solve your skin issues. You may also want to see a dietitian, who can help you find sources of gluten in your favorite foods and then search out alternatives.
Here are some dermatitis herpetiformis self-care tips that experts recommend to help you get started on your gluten-free life:
Focus on eating whole foods without gluten that you love. This could include vegetables, fruits, poultry, meat, fish, eggs, dairy, beans, nuts, and seeds. You can also eat grains that don't have gluten, such as quinoa, rice, and corn. Watch out for processed foods because these often have additives, flavors, and other ingredients that may make them unsafe for you to eat.
Make a list of all the foods with gluten you think you'll miss. You can often find specialty gluten-free foods to replace these. Many people follow a gluten-free diet these days, so there are plenty of products and recipes available to help you find new gluten-free favorites. If you're having trouble here, a dietician will probably have some helpful ideas and resources.
It is most common in people of northern European descent, where prevalence ranges from 1.2 to 39.2 per 100,000 people and an incidence range of 0.4-2.6 per 100,000 people per year. A recent large population-based study from the UK suggests that, although the incidence of GSE increased from 1990 to 2011, the incidence of dermatitis herpetiformis fell from 1.8 per 100,000 to 0.8 per 100,000 person-years over the same period. Seemingly, patients with dermatitis herpetiformis seem to have lower age-adjusted mortality than expected, possibly as a result of the modifications required to their diet as a result of the disease.
Multiple studies show that the disease is more common in men than women, with a male-to-female ratio of 1.5-2: 1.
This is a disease of people of northern European descent and is most uncommon in Asian and African populations, though a few cases have been reported. The incidence and prevalence of the disease are similar in North American populations of European descent to those seen in northern Europe, suggesting that genetic factors are important in disease susceptibility. Asian patients with dermatitis herpetiformis tend to have a distinct fibrillar pattern of IgA deposition in the skin, and there is a very rare association with GSE.
Associated Diseases

Dermatitis herpetiformis (DH) was described as a dermatological entity by Louis Duhring in 1884, 4 years before Samuel Gee defined the gastrointestinal symptoms of celiac disease [1, 2]. In the 1960s, small bowel biopsies taken from patients with DH showed villous atrophy in most patients, although they had no overt gastrointestinal symptoms [3, 4]. One-fourth of the patients with DH had normal small bowel villous architecture with an increased density of intraepithelial lymphocytes, which was later confirmed to be celiac-type minor enteropathy [5]. The finding of immunoglobulin A (IgA) deposits in the papillary dermis of patients with DH was of the utmost diagnostic importance [6]. In the 1970s, further findings linking DH and celiac disease included an identical human leukocyte antigen (HLA) pattern [7], the response of the rash to a gluten-free diet (GFD) [8, 9], and the occurrence of both diseases within families [10]. In the 1990s, genetic studies confirmed that virtually every patient with DH and celiac disease had the alleles contributing to the HLA-DQ2 or HLA-DQ8 haplotype [11], and even monozygotic twin pairs affected by both phenotypes were found [12].
DH is now known to be a common extraintestinal manifestation of celiac disease occurring in up to 10% of the celiac disease patient series in Europe and North America [13–15]. Small DH series have also recently been described in Brazil, China, and India [16–18]. The incidence of DH has been shown to be decreasing [19, 20], whereas the opposite is true for celiac disease, most likely because of improved awareness of subclinical cases and the wide use of serologic screening [21]. However, why only some undiagnosed celiac individuals develop an itchy blistering rash with dermal IgA deposits, i.e., DH, remains unknown.
During the last 20 years, several important research findings have emerged. A breakthrough in celiac disease research was the discovery by Dieterich et al. [22] in 1997 that tissue transglutaminase (TG2) was the target autoantigen for IgA antibody responses. Five years later, Sárdy et al. [23] showed that epidermal transglutaminase (TG3) was the autoantigen in DH. At present, IgA-class TG3 autoantibodies are known to be produced by plasma cells in the small bowel [24], they occur in the blood of most patients with DH, are partly bound in the circulating immune complexes, and disappear with a GFD [25, 26]. Importantly, the TG3 enzyme coexists with IgA autoantibodies in the dermal deposits, forming tightly bound immune complexes [27].

