
Winkelwagen
U heeft geen artikelen in uw winkelwagen
Histopathology of mycosis fungoides varies within stages of the disease. Superficial lymphoid infiltrate, epidermotropism with absent or rare spongiosis spongiosis, and lymphoid atypia are the predominant features.[4][15][16]
Patch stage: In the early patch stage. it may be difficult to diagnose as infiltrates may be very scant. In more established patches, a lymphocytic infiltrate may be seen around the basal cell layer. The cells are usually small, well-differentiated lymphocytes with rounded or cerebriform nuclei. The epidermis shows hyperkeratosis and acanthosis. Basal cell degeneration with melanin pigment incontinence may be seen. A dense, mixed perivascular infiltrate may be seen, along with fibrosis of dermal papillae.
Plaque stage: In the plaque stage, the epidermis shows acanthosis with a psoriasiform hyperplasia and absent or rare spongiosis. The upper dermis may show a dense, band-like lymphocyte infiltrate with cerebriform nuclei and prominent epidermotropism. A third of cases may show Pautrier's abscesses.
Tumor stage: A loss of epidermotropism may be noticed in the tumor stage. The infiltrate is a dense dermal infiltrate with large cerebriform lymphocytes, with a diminished number of T lymphocytes and dendritic cells.
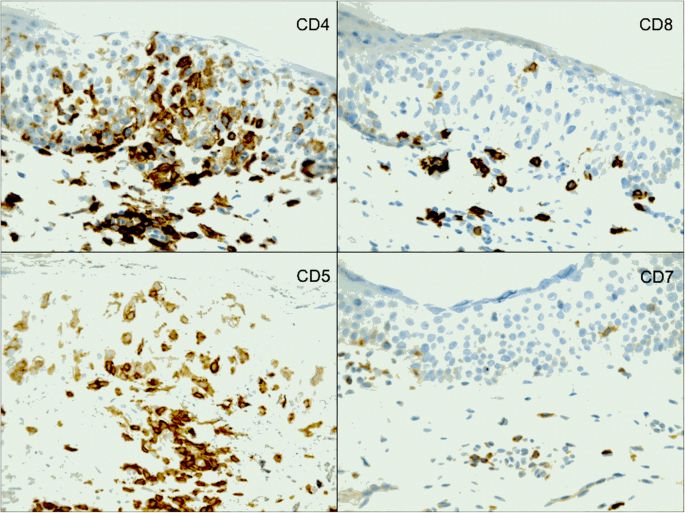
Immunohistochemistry
Mycosis fungoides tumor cells are characterized by epidermotropic peripheral T lymphocytes whose phenotype is CD2+, CD3+, CD4+, and CD5+. In a minority of patients with mycosis fungoides, T lymphocytes may be CD4- and CD8+, CD4- and CD8-, or CD4+ and CD8+.[15]The loss of CD7 expression can be observed even in the early phases of the disease. However, isolated negativity for CD7 is not a sufficient criterion for diagnosis as it can be shown in inflammatory dermatoses. The loss of CD26 expression seems to be specific to mycosis fungoides neoplastic cells.[17]
The immunohistochemical pattern of Sezary syndrome is CD3+, CD4+, CD7-, and CD8- cells, which is identical to mycosis fungoides. Immunostaining for MUM-1 (multiple myeloma oncogene) might be used to differentiate these as it is positive in Sezary syndrome and negative in mycosis fungoides.[17]
Psoriasis is een chronische, inflammatoire huidziekte die 2–3 % van de populatie treft. Psoriasis is geassocieerd met vele comorbiditeiten, waaronder artritis psoriatica, cardiovasculaire aandoeningen en depressie. Daarnaast kan er sprake zijn van sociale problematiek en wordt de levensloop van patiënten met ernstige vormen op negatieve wijze beïnvloed. Psoriasis wordt gekenmerkt door rode, schilferende plaques die gepaard gaan met jeuk. Op kinderleeftijd kan het klinisch beeld op eczeem lijken. Er zijn veel (nieuwe) effectieve behandelopties voor psoriasis, waaronder biologics en small-molecule inhibitors. Er zijn duidelijke aanwijzingen dat psoriasis bij vrouwen een grotere invloed heeft op hun kwaliteit van leven dan bij mannen. Behandeldoelen lopen eveneens uiteen tussen beide seksen. Vrouwen stoppen vaker met biologics in verband met de bijwerkingen, en zijn minder vaak tevreden over de behandeleffecten. Therapiekeuze rond kinderwens en zwangerschap vraagt maatwerk, voor vrouwen én mannen. Aandacht voor genderspecifieke aspecten bij de behandeling van patiënten met psoriasis is daarom belangrijk.
This is a preview of subscription content, log in via an institution to check access.
‘Wat zie je?’ is een vraag die velen met moeite beantwoorden. Het is immers niet makkelijk een visuele waarneming objectief te beschrijven, zonder te interpreteren wat je ziet. Of het nu bij je coschap dermatologie of huisartsgeneeskunde is, deze vaardigheid is relevant bij ieder vak waarbij inspectie van belang is.
Het lichamelijk onderzoek en beschrijven van huidafwijkingen en huidziekten kan uitdagend zijn. Tegelijkertijd kan een simpele blikdiagnose de valkuil hebben dat je belangrijke overwegingen mist. Om die redenen is het aan te raden een vaste systematiek te hanteren bij de beoordeling van huidafwijkingen. Het meest gebruikte hulpmiddel daarvoor is het welbekende acroniem ‘PROVOKE’. Na dit artikel beheers je de basis hiervoor. De volgende keer dat iemand je vraagt ‘wat zie je?’, hanteer je deze leidraad en loop je de huidinspectie gericht en systematisch door.
P: handruggen
R: gegroepeerd
O: lenticulair tot nummulair, tiental
V: rond, vlak
O: matig scherp begrensd
K: erythemateus
E: plaques
Dus: op beide handruggen een tiental lenticulaire tot nummulaire ronde vlakke matig scherp begrensde erythemateuze plaques.
Diagnose: handeczeem, bijvoorbeeld atopisch of ortho-ergisch (irritatief).
P: linkerneusvleugel
R: solitair
O: lenticulair
V: rond, opgeworpen rand
O: scherp begrensd
K: glanzend erythemateus
E: papel
Dus: op de linkerneusvleugel een solitaire lenticulaire scherp begrensde ronde glanzende erythemateuze papel met opgeworpen rand.
Diagnose: basaalcelcarcinoom.
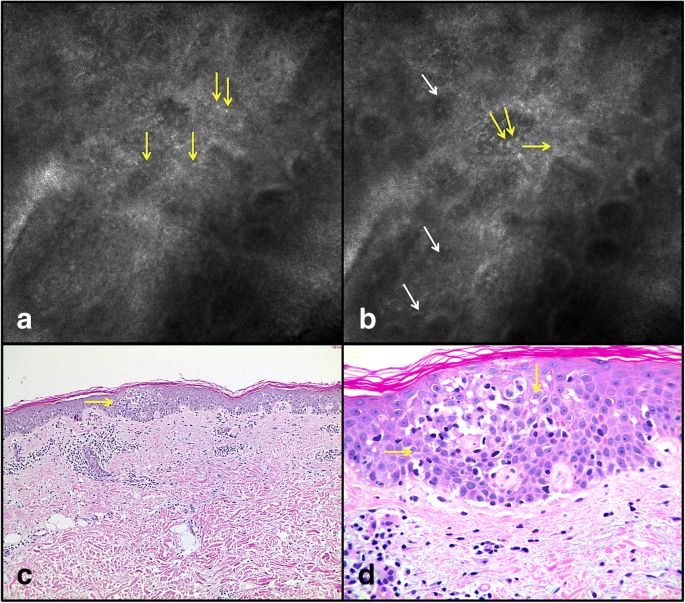
The histopathology exam, complemented by immunohistochemistry, is still the gold standard for the diagnosis of MF, and it’s based on the presence of atypical lymphocytes with cerebriform nuclei, surrounded by clear cytoplasm, arranged in band in the papillary dermis and in the DEJ. In early stages of MF, histopathologic findings can simulate inflammatory diseases, presenting only with reactive lymphocytes and with absence of lymphocytic cytologic atypia, as seen in this clinical presentation. Pautrier micro-abscesses are cluster of atypical lymphocytes in an epidermotropism distribution. Pautrier micro-abscesses are the pathognomonic findings in the histopathology exam of MF, but are only seen in 25% of cases, present mostly in advanced lesions of plaque-stage MF [1, 3]. Furthermore, there is also great heterogeneity between the lesions: two or more simultaneous biopsies in different suspicious lesions usually reveals different histopathological aspects.
Previous studies have evaluated reflectance confocal microscopy (RCM) as a promising tool for MF diagnosis because it offers the unique opportunity to analyze skin structures non-invasively at a ‘quasi-histopathologic’ resolution and to guide the most representative site for the biopsy [3, 4].
Koller et al.l reported that RCM examination of MF lesions revealed an interface dermatitis and an infiltration of the upper epidermal layers by roundish cells, distributed in nests or diffusely widespread throughout the epidermis. These authors referred a sensitivity of 63,33% and a specificity of 92,89% for MF diagnosis and concluded that RCM can be used as a supportive tool to determine the best location for taking a punch biopsy [5].
Li et al. reported a series of RCM features of MF which showed correlation with histopathological evaluation, from 10 patients with MF. In this study, dermal papillary rings were weak reflected light in all skin lesions evaluated and the authors believed that it occurs due to infiltration of atypical lymphocytes. Disarray of honeycomb of stratum, round to oval cells diffusely widespread throughout the epidermis and in the papillary dermis, infiltration of inflammatory cells in superficial dermis were others features reported [4].