
Winkelwagen
U heeft geen artikelen in uw winkelwagen
If a skin biopsy does not indicate leukocytoclastic vasculitis, consider these differential diagnoses 1 :
The management and treatment of leukocytoclastic vasculitis is dependent on the causes or triggers and whether there is systemic involvement.
For cutaneous leukocytoclastic vasculitis, the treatment is largely focused on symptom management. Providers should direct all patients with leukocytoclastic cutaneous vasculitis to elevate the affected areas, utilize compression socks, and minimize walking or standing. 6
In most cases, the episodes are acute and resolve on their own—especially if they are due to a medication. However, some patients may experience recurrent episodes that follow different patterns with flare-ups that are occasional, intermittent, or constant. Recurrence is more likely if the trigger is unknown. Eliminating the trigger will often prevent recurrence in cases with an identifiable cause.
Pharmacological interventions can be used for cutaneous leukocytoclastic vasculitis when necessary. However, the protocol and dosages vary depending on the extent of the condition and the specific needs of the patient. Corticosteroids are the standard pharmacological option for skin-limited leukocytoclastic vasculitis. For long term management, colchicine may be an option. Dapsone, hydroxychloroquine, and nonsteroidal anti-inflammatory drugs (NSAIDs) may also be considered based on limited evidence. 6
Corticosteroids are also the standard option for cases with systemic involvement and may be used with or without immunosuppressants, including azathioprine and methotrexate. Plasma-exchange or rituximab may be an option for more severe cases. 6
Therapy and monitoring depends entirely on the severity and extent of disease as assessed by body surface involvement, presence of ulceration, pain, neuropathy, joint pain or other systemic symptoms. Expensive or immunosuppressive medications other than prednisone are often not required in skin-only vasculitis and a rush to use these medications with only cutaneous disese is not needed.
Monitoring depends upon the drugs used in therapy and the severity of disease. Some forms of vasculitis, such as HSP, are notoriously slow to respond and may take several weeks to months to reach maximum improvement. Other forms of vasculitis not associated with any systemic disease may respond in days to weeks. Response to treatment may be assessed initially in days and should include a reduction in new lesion formation, pain or neuropathy. Patients need to be followed closely and at least weekly until response is assured and then less often.
Changes in therapy depend upon response, lack of it or finding of other organ involvement, such as renal.
Patients who are otherwise healthy coming into an episode of cutaneous vasculitis most often will tolerate the disease as well as most any of the treatments discussed above. Special circumstances include the presence of diabetes or other immune-suppressing premorbid conditions such as chronic lymphocytic leukemia (CLL). In these diseases nonsteroidal options may be. HSP is also known to recur, and renal abnormalities may present weeks to months after the initial episode of cutaneous vasculitis. Therefore, special scrutiny of general health issues, including presence of malignancy and assessment of renal function, are appropriate especially in adults with chronic (months) or recurrent disease.
A rare form of cutaneous vasculitis in children is known as acute hemorrhagic edema (AHE) of infancy. Most consider AHE to be in the spectrum of IgA vasculitis but differentiated by the young age of patient (most often 2 years or less), characteristic urticarial-like skin lesions of the feet or legs and face and no systemic complications. As is true with HSP, it is preceded by a viral or bacterial illness, but renal disease is not seen and the course is self-limited.
Leukocytoclastic vasculitis (LCV) is a histopathologic description of when vasculitis occurs in the small vessels of the skin or organs due to inflammation caused by neutrophils with leukocytoclasia. 1
There is significant confusion around the naming of leukocytoclastic vasculitis. It is often misused as a descriptor of a specific disease or type of vasculitis, when in fact it is a histopathologic phenomenon that occurs with many different diseases. For example, leukocytoclastic vasculitis is sometimes mistakenly used as a label for the diseases it commonly coincides with, such as cutaneous small-vessel vasculitis and cutaneous leukocytoclastic angiitis. While leukocytoclastic vasculitis can be present in systemic diseases, it most often manifests cutaneously. 1
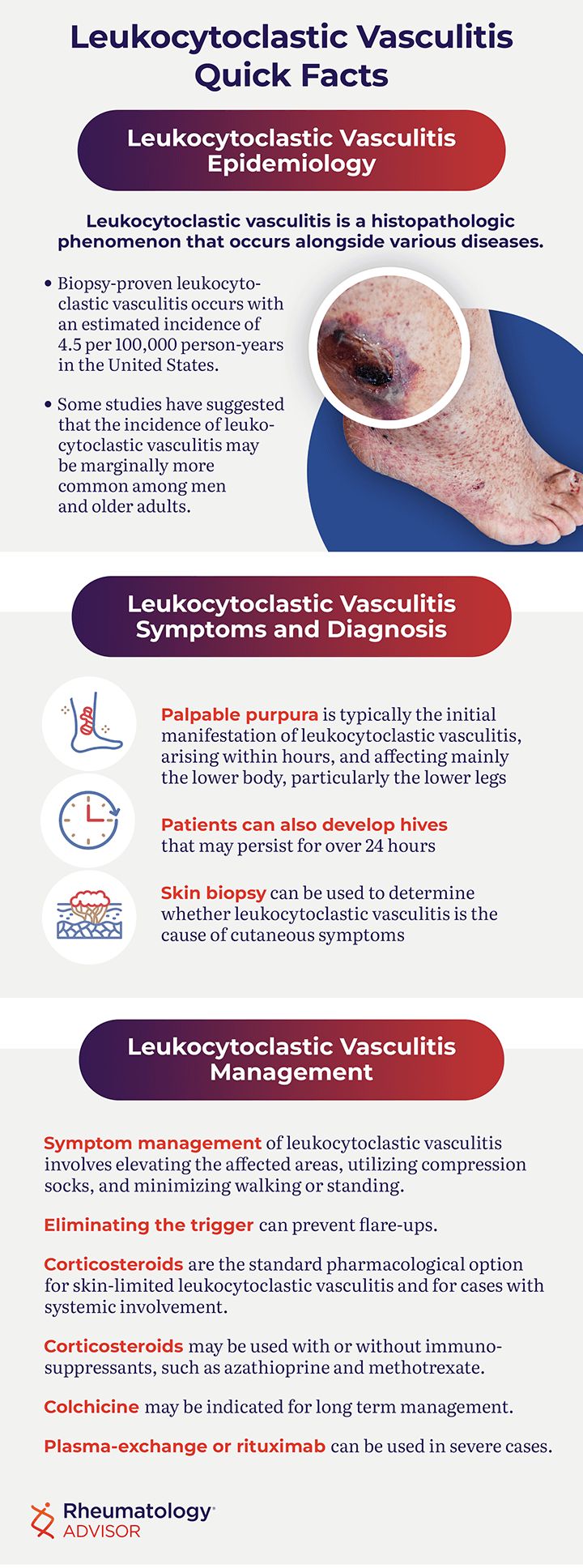
Since leukocytoclastic vasculitis is poorly defined, it is difficult to estimate the incidence and prevalence. Biopsy-proven leukocytoclastic vasculitis occurs with an estimated incidence of 4.5 per 100,000 person-years in the United States. 1 Research estimates the prevalence in different locations to range from 2.7 to 29.7 per million. 1
The incidence of leukocytoclastic vasculitis seems to be evenly distributed across different ages and genders. However, some studies have suggested it may be marginally more common among men and older adults. 1,2
Patients with “idiopathic” cutaneous LCV may exhibit various disease patterns. Most cases self-resolve within 3-4 weeks. Some patients may flare only intermittently, perhaps for 2 weeks every other year, others have recurrent flares every 3-6 months or intractable disease with new lesions almost every day or week for years.
Identifying and controlling triggers or exacerbating factors such as prolonged standing, alcohol use, or specific drug use can help, as can wearing compression stockings and keeping the feet elevated. Bed rest can accelerate the regression of skin lesions but is rarely feasible in active patients.
Topical treatments such as emollients or corticosteroid creams are sometimes prescribed and may transiently alleviate pruritus when present. The efficacy of such treatments is not supported by any data and is highly variable.
Systemic pharmacological therapies should be considered after careful discussion with the patient and should be driven by the frequency of flares, the associated discomfort, and the psycho-social impact of the disease. Several different agents must often be tried before finding one that will help limit the frequency and/or intensity of the disease, and for many patients, cure remains an elusive goal.
Although cutaneous small-vessel vasculitis is not rare, few epidemiological studies and no large controlled therapeutic trials have been conducted. Short courses of systemic glucocorticoids can be prescribed for severe flares of cutaneous disease (prednisone, 0.5 to 1 mg/kg/day for 1 week, followed by a rapid tapering over 2-3 weeks). However, the response is not universal and usually requires relatively high doses, so recurrence with tapering and glucocorticoid-dependency are common. Out of concern for adverse side effects, glucocorticoid therapy should be avoided for skin-limited disease except for short periods.