Winkelwagen
U heeft geen artikelen in uw winkelwagen
Lupus erythematosus tumidus (LET) is a chronic relapsing inflammatory disease of the skin and was first described by Erich Hoffmann in 1909, 1 presenting two patients with rounded, elevated, erythematous and non-scaling urticarial lesions. This article was followed by a report in 1930 with subsequent reports describing LET in the 1950s. 2 , 3 LET occurs predominantly on sun exposed areas. Sometimes the skin lesions have an annular or semi-annular (“arciform”) appearance but there are no epidermal changes and therefore no scale, ulceration or crust formation. Every lesion heals without scarring or postinflammatory hyper- or hypopigmentation and therefore LET does not result in chronic skin damage. 4 ( Figure 1 )
Clinical picture of Lupus erythematosus tumidus: erythematous, urticarial plaque and papules on the neck of a 43-year old male smoker. Consent was received for the publication of this image.
The high photosensitivity of LET patients and the evolution of standardized photoprovocation protocols has helped to improve the scientific evaluation and identification of the disease in recent years. 5 – 7 The development of histologic and immunohistologic evaluation procedures supported important similarities with other forms of cutaneous lupus erythematosus (CLE) and has resulted in a better differentiation of LET from other CLE subtypes at the microscopic level. 8 – 10 This has substantially increased awareness of LET, resulting in a higher reporting rate in the literature.
Duesseldorf classification of cutaneous lupus erythematosus (CLE) a
| Acute cutaneous lupus erythematosus (ACLE) |
| Localized form |
| Generalized form |
| Subacute cutaneous lupus erythematosus (SCLE) |
| Annular form |
| Papulosquamous form |
| Chronic cutaneous lupus erythematosus (CCLE) |
| Discoid lupus erythematosus (DLE) |
| Localized form |
| Disseminated form |
| Lupus erythematosus profundus (LEP) |
| Chilblain lupus erythematosus (CHLE) |
| Intermittent cutaneous lupus erythematosus (ICLE) |
| Lupus erythematosus tumidus (LET) |
Keinesfalls sollte eine Schwangerschaft während eines Krankheitsschubs stattfinden, da dies die Komplikationsrate für Mutter und Kind erhöht. Kommt es zu einer Schwangerschaft während eines LE-Schubs, sollte unverzüglich die Zuweisung an ein spezialisiertes Zentrum erfolgen.
Screening-Methode der ersten Wahl ist das fetale EKG (erweiterte Methode des Tokogramms). Die therapeutischen Optionen reichen von plazentagängigen Steroiden bis hin zur Apherese [52]. Ro/SSA- beziehungsweise La/SSB-positive Schwangere sollten auch ohne Klinik präventiv Hydroxychloroquin erhalten [53].
Ein APLAS kann Aborte, Frühgeburten und (Prä-)Eklampsie auslösen. Mütter mit positiven Antiphospholipid-Antikörpern sollten auch ohne stattgehabtes klinisches Ereignis präventiv 100 mg Acetylsalicylsaure (ASS) erhalten [53].

In der Abklärung eines LE geht es aus dermatologischer Sicht immer um zwei Fragen:
In Bezug auf Hautveränderungen im Rahmen eines LE wird zwischen LE-spezifischen Veränderungen (CLE) und solchen, die auch bei anderen Kollagenosen vorkommen können, unterschieden.
Die zwei wichtigsten Klassifikationen des CLE sind jene von Sontheimer und Kuhn (Tab. 1) [29, 30].
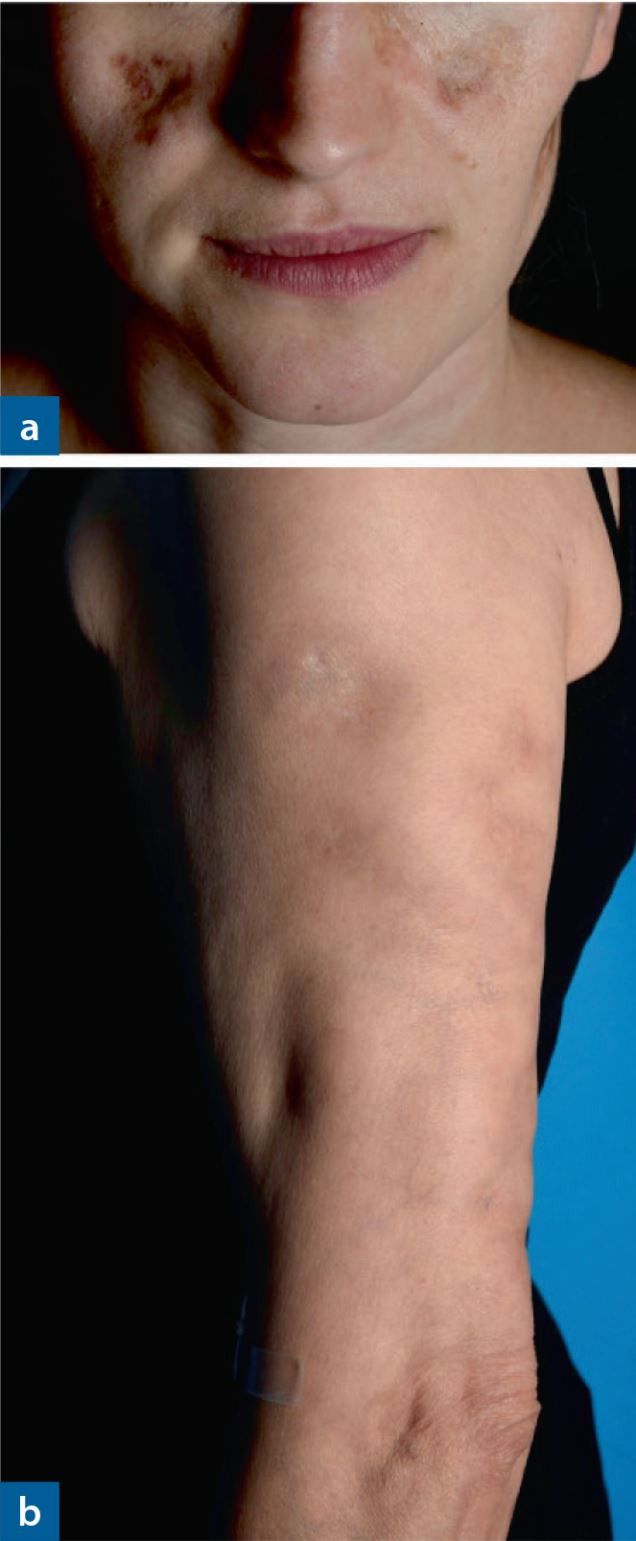
Andere Erscheinungsformen des CCLE an der Haut sind zum Beispiel die Lupus- Pannikulitis (Abb. 6), der "mucosal CCLE" oder der an Frostbeulen erinnernde und akral (Finger, Zehen, Nase, Ohren) auftretende Chilblain-Lupus (Abb. 7).
Der CCLE hat eine geringe Wahrscheinlichkeit (ca. 5 %), im weiteren Verlauf einen SLE zu entwickeln. Der SCLE ist überdurchschnittlich lichtempfindlich und ebenfalls durch schuppende, erythematöse, jedoch meist anulär angeordnete Plaques gekennzeichnet (anulärer SCLE, Abb. 8). Eine weitere Spielart des SCLE ist der psoriasiforme SCLE. Die Herde des SCLE entwickeln sich rascher als beim CCLE, gelegentlich so rasch, dass die Schuppung als Zeichen der Chronizitat fehlt. SCLE-Herde treten ebenfalls bevorzugt in den UV-exponierten Arealen auf. Auch die Histologie entspricht im Wesentlichen (abgesehen von der Vernarbung) der des CCLE. Der SCLE ist häufiger (ca. 25 %) mit einem SLE assoziiert als der CCLE. Eine deutliche Assoziation besteht auch mit Ro/SSA beziehungsweise La/SSB-Autoantikörpern.