
Winkelwagen
U heeft geen artikelen in uw winkelwagen
Take a quiz to find out what's causing your redness.
The cause is believed to be a congenital abnormality that leaves the testicle insufficiently anchored within the scrotum.
Most susceptible are infant boys and boys just reaching puberty. Torsion may occur in older boys after an injury and/or an athletic workout.
Symptoms include sudden, severe, one-sided testicular pain and swelling, with nausea and vomiting.
Diagnosis is made through physical examination and sometimes ultrasound.
Treatment involves first attempting to manually rotate the testicle back into place. If unsuccessful, surgery will be done to either correct the torsion or to remove the testicle if the damage is not reversible.
Scabies is a rash caused by the microscopic human itch mite. It burrows into the top layer of skin to feed and causes severe itching and irritation.
Symptoms include intense itching, especially at night, and a rash of tiny red bumps. Scratching may cause the rash to form sores, scales, or crusts. The rash most often forms between the fingers, in the folds of the wrists and elbows, and any place normally covered by clothing.
It is important to get treatment because the scratching can cause an infection in the skin. In children, mites can cover nearly the entire body.
Diagnosis is made through physical examination and skin test.
Rarity: Rare
Top Symptoms: vaginal itch or burning, vulvovaginal redness, feeling itchy or tingling all over, butt itch, elbow itch
Urgency: Primary care doctor
Most susceptible are those with weakened immune systems, though anyone can contract ringworm.
Redness (also known as erythema) of the skin is the result of increased flow in the blood vessels close to the skin that occurs in the setting of injury, infection or generalized inflammation. There are many things that may cause a red scrotum, so it is important to seek medical attention for proper diagnosis.
Inflammatory causes of scrotal redness can be related to the following.
Proper hygiene is key in maintaining genital health. Regularly cleaning underneath the foreskin of the penis and around the scrotum with mild soap and water is very important in keeping harmful bacteria away. It is also important to practice good sexual hygiene. Using condoms and limiting the number of sexual partners is essential in preventing the transmission of sexually transmitted infections.
Being exposed to allergens can easily irritate this sensitive area of the body.

A 57-year-old man presented to our department because of persistent redness of the scrotal skin and the base of the penis for about two years. He had suffered from severe itching intertriginous eczema and anal pruritus with anal fissures for more than 20 years. He had been treated with topical corticosteroids and topical antimycotics. Because of the chronic anal fissuring he was treated with botulinum A injections in the anal spincter and surgical fissure ectomy. He was taking an oral statin to control hypercholesterinemia for several years.
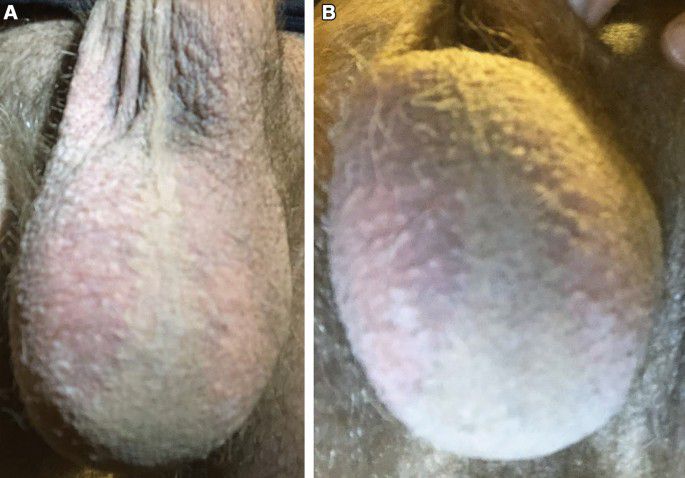
On examination we found a healthy man with a highly erythematous scrotal skin without any significant scaling, infiltration or lichenification. There was a sharp border to the adjacent unaffected skin [ Fig. 1 ]. On the inner thighs striae were present due to long-term steroid application.
Red scrotum syndrome. (A) Sharp border between intense erythematous scrotal skin and adjacent skin. No scaling. (B) Less intense redness on the posterior site.
We made the diagnosis of RSS. He was given topical corticosteroid ointments without improvement. Even two courses of systemic corticosteroids did not improve the situation. There was an improvement of the erythema after several weeks due to topical calcineurin inhibitor pimecrolimus. The burning and sometimes itching sensations and the hyperalgesia the patient experienced did not improve much. After 4 months, however there was a relapse that could not be controlled by pimecrolimus ointment anymore. Oral doxycycline for 4 weeks did not result in any improvement. Therefore, treatment was switched to oral gabapentine. After 2 weeks a partial remission was noted and further improvement was observed during the next 2 months.
The diagnosis of RSS was made. We started treatment with doxycycline p.o. and tacrolimus 0.1% ointment twice daily with a complete remission of his burning sensations. The redness also improved markedly within 10 days. After 4 weeks treatment was stopped because of complete remission. Both patients reported lower back pain and lumbago in the past but they did not connect these complaints to the scrotal skin affection.

Risk factors for getting intertrigo include:
There are several things you can do to try to prevent getting intertrigo, including:
If you’ve had repeated cases of intertrigo, the following actions may help to prevent future cases:
While intertrigo can be unpleasant and painful, it is treatable. The prognosis (outlook) for intertrigo depends on the person’s overall health. In most cases, people recover well from intertrigo if it’s treated properly.
Intertrigo can become chronic (long-lasting) or recurrent (occurring often), so it’s important to take care of yourself and follow a proper hygiene routine to prevent your intertrigo from coming back.
If intertrigo is not treated properly, it can cause complications, including:
At condition onset, the patient was a 26-year-old man with a history of recurrent tinea versicolor affecting the trunk and neck and no other significant medical history, including no history of topical corticosteroid use. He experienced the abrupt onset of erythema of the bilateral scrotum accompanied by intense itching and burning. The signs and symptoms began one morning following sexual intercourse with a female partner the previous night. The patient did not clean up after intercourse and fell asleep lying on his back with vaginal secretions covering his scrotum.
On examination, the erythema was well-demarcated, closely following the distribution of hair on the bilateral scrotum and also involving a small portion of the hair-covered ventral shaft of the penis. There was sparing of erythema along the hairless portion of the scrotal midline and the hairless underside of the scrotum (Fig. 1). There was no evidence of ulceration or swelling, and there was no tenderness on palpation of the affected area. The patient first sought care with his primary care physician, where HIV testing and HSV 1 and 2 serum antibody testing were performed and were all negative. The patient then completed a 4-week course of topical clotrimazole cream with no improvement in symptoms. A 10-day course of erythromycin was also tried under the assumption that the condition represented an atypical presentation of erythrasma, but also with no improvement.
During this time the patient experienced significant psychological distress, including decreased concentration, insomnia, anhedonia, decreased libido, and decreased appetite with weight loss. Seeking further assistance, the patient sought the opinion of a private practice dermatologist, who had previous experience as a military physician. That dermatologist acknowledged that he had seen about a dozen cases of RSS previously and advised that from his experience only about half of patients experience improvement. Additional treatments were attempted including pulsed dye laser therapy (targeted at hypervascularity) and liquid nitrogen cryotherapy, neither of which provided improvement. An extended course of minocycline was also attempted, but the patient had to discontinue the drug after several days due to intolerance (metallic taste).