
Winkelwagen
U heeft geen artikelen in uw winkelwagen
A 49-year-old female with a body mass index of 17 kg/m 2 presented for pathological fracture of right femoral bone head with metastatic adenocarcinoma and was scheduled to undergo bone tumor resection and artificial bone replacement. She was diagnosed with Osler-Weber-Rendu syndrome at the age of 30 and accompanied with multiple pulmonary arteriovenous malformations (AVMs) and pheochromocytoma. She had a history of brain abscess, takotsubo cardiomyopathy and preoperative coil embolization of the AVMs. She did not have any history of recurrent epistaxis or gastrointestinal bleeding.
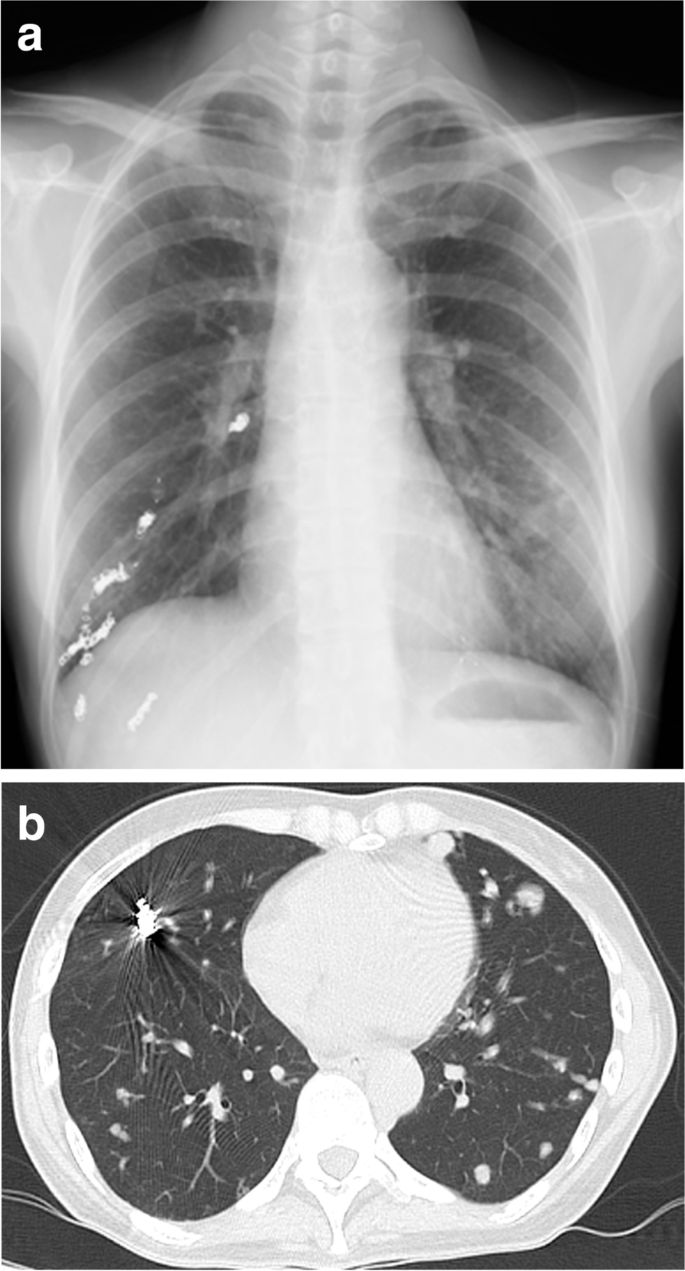
A preoperative physical examination did not reveal any special finding on her body surface. Blood pressure was 105/64 mmHg, with doxazosin at a dose of 3 mg per day, and heart rate was 97 bpm. Peripheral oxygen saturation (SpO2) was 86% in room air, possibly due to the remaining pulmonary AVMs, but the Hugh-Jones classification was class I. Blood tests were remarkable only for hemoglobin level of 11.2 g/dL. Urinary adrenaline, noradrenaline and dopamine levels were 14.2 mcg/day, 965.8 mcg/day and 807.3 mcg/day, respectively. An electrocardiogram (ECG) showed negative T-waves on V3-5 and a transthoracic echocardiogram showed a peripheral left ventricle hypertrophy with an ejection fraction of 67%. Preoperative image examination revealed bilateral pulmonary AVMs (Fig. 1a, b), but no AVM in the brain or in the spinal cord, and a pancreas tail tumor, which was considered to be the origin of the metastatic bone tumor.
Preoperative estimation of the operation duration was 5 h, and estimated intraoperative blood loss was 500 mL. She was in anxiety and wished to have sedation during the procedure.
Combined spinal and epidural anesthesia was planned in order to reduce the risk of rupture of the pulmonary AVMs due to inadequate pain control and positive pressure mechanical ventilation. We planned to add sedation by general anesthesia with a supraglottic airway device (SGA) to maintain spontaneous ventilation because of the estimated long duration of surgery, her mental status and large amount of blood loss.
Bij ROW zijn meestal meerdere behandelingen mogelijk. Welke in uw situatie geschikt zijn, hangt onder meer af van de plek waar de klachten optreden. U vindt alle behandelingen hieronder, gesorteerd op de plaats van de klachten.
Als er vaatafwijkingen in de hersenen worden gevonden, dan wordt bekeken of behandeling nodig is. Dit hangt af van de grootte en de opbouw van de afwijking. Heel kleine afwijkingen hebben geen behandeling nodig.
Radiochirurgie
Wanneer wél behandeling nodig is, wordt soms de voorkeur gegeven aan bestraling. Dit duurt 20 tot 30 minuten en een eenmalige behandeling is vaak voldoende. Bij deze behandeling wordt de plek waar de vaatafwijking zit vanuit diverse richtingen bestraald met een relatief hoge dosis. Met deze techniek komt de vaatafwijking in het brandpunt van de bestraling te liggen en wordt het rondom liggende hersenweefsel vrijwel niet aangetast. Zo nodig kan de behandeling worden herhaald.
De kans op genezing met deze behandeling is 80% (na 1 tot 2 jaar). De kans op complicaties is kleiner dan 3% en eventuele complicaties zijn meestal van tijdelijke aard.
Operatie en/of embolisatie
Andere behandelingsmogelijkheden zijn operatie en embolisatie. Dit is een behandeling van een AVM, waarbij de slagader die het bloed aanvoert wordt afgesloten. Het afsluiten gebeurt door spiraaltjes of een plug in het bloedvat te plaatsen. Dit leidt tot de vorming van bloedstolsels die de slagader ter plaatse afsluiten waarbij de toevoerende slagader van binnenuit wordt afgesloten via een katheter die in de lies wordt ingebracht.
’Wil ik het wel weten?’
De wetenschap dat u een vaatafwijking in de hersenen heeft is vervelend, terwijl de kans op een bloeding betrekkelijk klein is. Maar hoe jonger u bent, hoe groter die kans wordt, omdat u nog vele levensjaren voor de boeg heeft. Daarnaast is de kans op een hersenafwijking groter als u ROW type 1 heeft, als u epilepsie heeft of regelmatig last heeft van hoofdpijn.
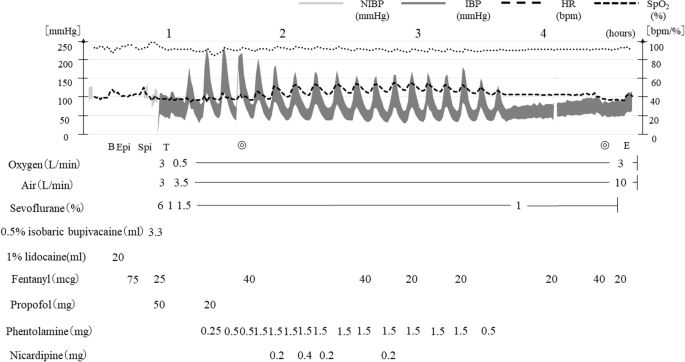
For selecting an anesthesia technique, the risks of general anesthesia and regional anesthesia as discussed above should be balanced with consideration of factors from the surgical procedure. We performed spinal and epidural anesthesia in order to avoid positive pressure ventilation and to provide adequate analgesia for a prolonged duration of surgery. Considering the possible long operation duration with the lateral position on the left side and with a risk of bleeding in the surgical field, sedation during the procedure was preferable. We decided to use sevoflurane with an SGA device to ensure spontaneous ventilation. While the use of an SGA device has a risk of upper airway bleeding, it enables possible emergent tracheal intubation through the laryngeal mask, even in the lateral position, in the case of respiratory and/or circulatory collapse during the procedure.
In summary, anesthesia management for Osler-Weber-Rendu syndrome is challenging. Both general anesthesia and neuraxial anesthesia including spinal and/or epidural anesthesia have advantages and disadvantages. For surgery with a long duration in the lateral position, neuraxial anesthesia combined with general anesthesia using an SGA device to maintain spontaneous ventilation could be an option.
Early diagnosis of HHT is based on clinical findings. Genetic testing helps confirm the diagnosis but is not required for an index case unless 1) they are children who have not developed all the clinical features or 2) to test at-risk family members and identify a family-specific mutation. Screening and treatment of visceral AVMs depend on the potential for high-risk complications. For instance, proactive screening and treating asymptomatic pulmonary AVMs are encouraged compared to asymptomatic hepatic or cerebral AVMs.[25]
HHT can affect multiple organ systems, and early recognition and screening for clinical manifestations and prompt interventions can decrease morbidity and mortality. Epistaxis is one of the most common presenting symptoms. Patients with HHT benefit from a multidisciplinary approach and should ideally be referred to a center specializing in HHT.

Hội chứng Osler-Weber-Rendu là một rối loạn ảnh hưởng đến mạch máu với biểu hiện và triệu chứng đa dạng từ giãn mao mạch trong mũi đến xuất huyết ở nhiều cơ quan khác nhau. Đây là một bệnh lý phức tạp, có ảnh hưởng không chỉ đến sức khỏe mà còn đến chất lượng cuộc sống của người bệnh.
Dấu hiệu phổ biến nhất của giãn mao mạch xuất huyết di truyền là giãn các mao mạch trong mũi, gây ra triệu chứng chảy máu cam lặp đi lặp lại nhiều lần. Điều đáng chú ý là dấu hiệu đầu tiên thường xuất hiện ở độ tuổi dậy thì hoặc tuổi trưởng thành, độ tuổi trung bình của lần chảy máu cam đầu tiên thường là 12 tuổi.
Bên cạnh đó, tình trạng chảy máu có thể xảy ra hàng ngày hoặc mỗi tháng một lần, chiếm khoảng 50 đến 80% số bệnh nhân bị bệnh giãn mao mạch xuất huyết di truyền. Biểu hiện của giãn mao mạch cũng xuất hiện ở các bộ phận khác của cơ thể, thường rõ ràng hơn ở những người trong độ tuổi từ 20 đến 40 tuổi.
Các đặc điểm của giãn mao mạch trên da và niêm mạc bao gồm các đốm nhỏ màu đỏ đến tím hay các đường ren đỏ sẫm, xuất hiện ở nhiều nơi như mặt, bên trong miệng, lỗ mũi, môi, tai, kết mạc mắt, cánh tay, bàn tay và ngón tay nhưng thường hiếm hơn so với hiện tượng chảy máu mũi.
Các tổn thương ban đầu có thể rất nhỏ, dần trở nên rõ ràng hơn ở cuối độ tuổi trưởng thành. Mặt khác, không chỉ giãn mao mạch mà còn các mạch máu hình thành bất thường xảy ra ở nhiều cơ quan khác nhau như hệ thống tiêu hóa, phổi, hệ thống thần kinh trung ương.
Xuất huyết tiêu hóa là một biến thường gặp, đặc biệt ở những người trên 50 tuổi, biểu hiện dưới dạng phân đen, kèm máu hoặc nôn ra máu. Ngoài ra, dị tật động tĩnh mạch ở phổi và não cũng có thể gây ra các vấn đề sức khỏe nghiêm trọng nếu bệnh không được quản lý, kiểm soát tốt.
The case was a 49-year-old female with Osler-Weber-Rendu syndrome, multiple pulmonary arteriovenous malformations and pheochromocytoma who presented for femoral bone head fracture with metastatic adenocarcinoma. The patient was scheduled to undergo bone tumor resection and artificial bone replacement, being positioned laterally with a planned operation duration of 5 h. Anesthesia was managed with spinal and epidural anesthesia, combined with sedation by sevoflurane using a supraglottic airway (SGA) device under spontaneous breathing. Her intraoperative and postoperative courses were uneventful.
Neuraxial anesthesia combined with general anesthesia using an SGA device to maintain spontaneous ventilation in order to minimize the risk of rupture of pulmonary arteriovenous malformations could be an option.