Winkelwagen
U heeft geen artikelen in uw winkelwagen
A thorough medical exam can help rule out possible causes, such as an infection or medication, which could be causing your hives.
It’s also possible for a disease, such as a thyroid condition, rheumatoid arthritis, or diabetes to cause hives. If signs indicate that this may be the cause, medical testing can find or rule out these causes.
The pressure of a purse strap can cause chronic hives where the strap rests on your body.
With so many possible causes, it’s easy to feel overwhelmed. The good news is that treatment can keep hives under control. Sometimes, it just takes time to find the treatment that works for you.
The American Academy of Dermatology gratefully acknowledges the support from Sanofi and Regeneron.
Diseases>Eczema>Sanofi-Regeneron Logo>2022" />
Hives are itchy welts on the skin. They can be caused by:
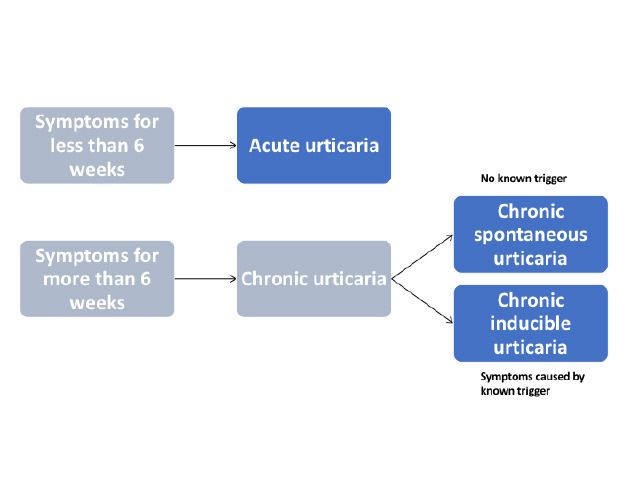
Regardless of what they look like, hives tend to appear and clear within a few hours. Some people have one flare-up and never get hives again. It’s also possible to have many flare-ups.
If you continue to get hives daily or almost every day for six weeks or longer, you have chronic hives. The medical term for this is “chronic urticaria."
When you have chronic hives, the most effective treatment often depends on the type of the hives you have and your medical history.

De typische urtica is een intens jeukende, scherpbegrensde verheven rode plek, welke vaak centraal bleek is. Afzonderlijke plekken kunnen groter worden en samenvloeien met andere plekken. Kenmerkend is dat ze binnen enkele uren verdwijnen zonder restafwijkingen aan de huid achter te laten.
Bij inspanningsurticaria ontstaan speldenknopgrote, jeukende of branderige rode bultjes. Deze treden op bij transpiratie, door lichamelijke inspanning of in een warme omgeving.
Urticaria factitia ontstaat in reactie op druk of wrijven van de huid. Hierbij ontstaan jeukende streepvormige kwaddels die na enige tijd weer spontaan wegtrekken. Met een stomp voorwerp krassend over de rug zijn ze reeds op te wekken. Dit verschijnsel noemt men ook wel positief dermografisme. Dit komt bij 3-5% van de bevolking voor in meer of mindere mate.
Bij vertraagde drukurticaria ontstaan na enkele uren pijnlijke, verharde zwellingen op drukplaatsen. Deze vorm ontstaat vaak rond de gewrichten en kan soms verward worden met een ontsteking van het gewricht. Behandeling van deze aandoening is erg moeilijk.
Urticaria wordt door artsen gemakkelijk herkend. De arts zal eerst vragen naar de meest voorkomende oorzaken. Het al pratend samen zoeken naar een mogelijke oorzaak leidt in een groot aantal gevallen tot de oplossing, zonder dat verder onderzoek noodzakelijk is. Pas wanneer er aanwijzingen zijn voor een mogelijke oorzaak, kan daar nog eventueel een gericht onderzoek naar worden gedaan.
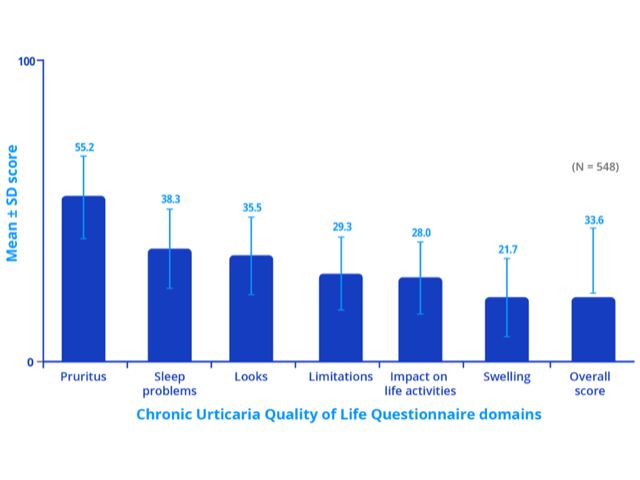
Patients with chronic spontaneous urticaria may experience sleep deprivation, anxiety, depression, lack of energy, and social isolation. These can result in a significant deterioration in the patient's quality of life (see figure 2). Chronic spontaneous urticaria is unpredictable and can disrupt the patient’s normal daily activities.
Figure 2 - Impact of chronic spontaneous urticaria on quality of life, sleep and daily activities
Note: Higher score indicates greater impairment of quality of life.
Credit: Adapted from Maurer M, et al. Allergy 2017, 72: 2005–16.
Recently, new guidelines have been published by the American Academy of Allergy, Asthma, and Immunology (AAAAI) and the European Academy of Allergy and Clinical Immunology (EAACI)/Global Allergy and Asthma European Network (GA 2 LEN)/European Dermatology Forum (EDF)/World Allergy Organization (WAO) that update what is currently understood about urticaria 3– 5 . There are several other published regional guidelines with similar recommendations, including Canadian 11 . With the exception of the American guidelines, the other organizations put forth a similar algorithm. That is, the following stepwise approach: first-line treatment includes second-generation H 1 antihistamines, second-line therapy involves up-dosing the second-generation H 1 antihistamine, and third-line treatment includes a new medication, omalizumab, which we recommend to be used before a more toxic medication, cyclosporine A.
The EAACI/GA 2 LEN/EDF/WAO guidelines do not include H 2 antihistamines in their algorithm due to a recent Cochrane review that shows lack of evidence of efficacy of these medications 13 . Thus, H 2 antihistamines are advised only on an individual case basis but not as first-, second- or third-line treatment. The AAAAI guidelines, however, consider the options of up-dosing second-generation H 1 antihistamines, adding other second-generation H 1 antihistamines, and adding H 2 antagonists, leukotriene receptor antagonists or first-generation H 1 antihistamines at bedtime to all be equally weighted second-line options 3 . In doing this, however, the adverse reaction profile would increase.
Both guidelines recommend that corticosteroids should be considered only for the short-term intervention and avoided as long-term treatments due to the significant number of side effects and alternative options for treatment. Both guidelines also acknowledge a role for cyclosporine A as an add-on treatment for patients who have refractory chronic urticaria that is not responsive to the above mentioned treatments 3, 5 .

Often the management for chronic inducible urticaria and chronic spontaneous urticaria will overlap.
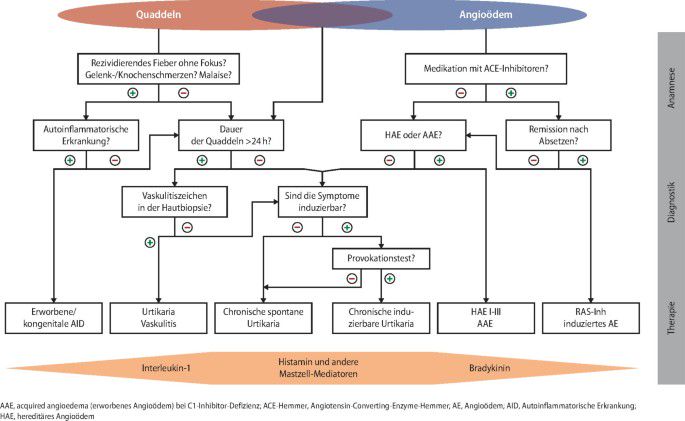
An algorithm for the symptomatic treatment of chronic urticaria is included in the international guidelines (see figure 4). The algorithm should be used with caution in children with chronic urticaria and in pregnant/lactating women as drugs contraindicated in pregnancy should not be used. Treatment should be continued until remission occurs.
Figure 4 - Pharmacological treatment algorithm for chronic urticaria
Many symptoms of urticaria are mediated by the actions of histamine on H1-receptors located on antihistamines is supported by clinical trial data. In some forms of physical urticaria, such as cold urticaria, ‘as required’ treatment may be appropriate.
Second-generation antihistamines are recommended in preference to first-generation antihistamines, as the latter have anticholinergic effects and sedative actions, and they interact with alcohol and many drugs that affect the central nervous system. Second-generation non-sedating antihistamines are the first-line symptomatic treatment for urticaria because of their good safety profiles. Those studied in the treatment of chronic urticaria include:
Terfenadine and astemizole are no longer available in New Zealand or Australia and should not be used as they are cardiotoxic in combination with ketoconazole or erythromycin.